Last reviewed May 10, 2026
Quick answer: Perimenopause fatigue isn't one thing. It's four distinct mechanisms — sleep architecture disruption, HPA-axis flattening, iron and ferritin depletion, and subclinical hypothyroidism — running in parallel and compounding each other. Each has a different treatment. Get the 4 specific lab tests (TSH + free T4, ferritin with target above 70 ng/mL, estradiol/FSH, AM cortisol) before you accept "just get more sleep." 32-40% of perimenopausal women experience moderate-to-severe fatigue (SWAN; Kravitz 2003). HRT addresses the sleep and HPA arms; ferritin and thyroid each need their own treatment.
The 60-second version
If you sleep eight hours and still wake up exhausted, this article is for you
You sleep eight hours. You wake up exhausted. You drink coffee. It does almost nothing — maybe takes the edge off, maybe gives you 90 minutes before the heaviness settles back in. By 11 a.m. you are running on fumes. By 3 p.m. you would put your head down on your desk if anyone would let you. You climb into bed at 9:30 p.m. because you are too tired to make it to 10. And the cycle starts again.
You are 47. Your doctor took your blood pressure, ordered a CBC, looked at the screen for ninety seconds, and told you to "manage your stress" and "exercise more." You walked out of that appointment knowing she was wrong but not knowing how to push back. You are not lazy. You are not deconditioned. You are not depressed — or at least, you weren't until the relentless perimenopause tiredness started making everything feel pointless. The bone-deep exhaustion is something else, and it has a specific name: perimenopause fatigue. If you typed why am I so tired in perimenopause into a search box at midnight last week, this article is the answer most clinicians do not have time to give you in a 10-minute appointment.
Most articles on this topic say "menopause fatigue is from poor sleep — get more sleep." That is wrong. The reality the literature actually supports is that perimenopause fatigue is not one thing. It is four distinct biological mechanisms running at the same time, often two or three of them compounding each other. Each one has a different treatment. Each one needs a different test. The reason "manage your stress" doesn't work is that it doesn't address any of them. This article is the workup most clinicians skip — and the four lab numbers you should walk into your next appointment with on a piece of paper.
Perimenopause fatigue is four distinct mechanisms — and most clinical reviews collapse them into one.
The Study of Women's Health Across the Nation (SWAN) — Kravitz et al. 2003 — followed 12,425 women across the menopausal transition and documented that 32-40% reported moderate-to-severe sleep complaints and fatigue interfering with daily function. Joffe et al. (2010) in Menopause showed the fatigue persists despite adequate sleep duration in a substantial subset of women, because the mechanism is disrupted sleep architecture, not insufficient sleep quantity. Schmidt and Rubinow's (1991) review of HPA-estrogen interactions, Punnonen and Rauramo's 1980 work on iron depletion in heavy perimenopausal bleeding, and Schindler's 2003 Maturitas paper on thyroid dysfunction in perimenopause round out the four-mechanism picture. Most contemporary reviews discuss one of these in isolation. The clinical reality is that two or three usually run in parallel, which is why a single-lever intervention so often fails.
Citations: Kravitz HM, et al. Sleep difficulty in women at midlife: a community survey of sleep and the menopausal transition. Menopause. 2003;10(1):19-28. PMID: 12544673 · Joffe H, Massler A, Sharkey KM. Evaluation and management of sleep disturbance during the menopause transition. Semin Reprod Med. 2010;28(5):404-421. PMID: 20613668 · Schmidt PJ, Rubinow DR. Menopause-related affective disorders: a justification for further study. Am J Psychiatry. 1991;148(7):844-852. PMID: 2026136 · Schindler AE. Thyroid function and postmenopause. Gynecol Endocrinol. 2003;17(1):79-85. PMID: 14559378.
The 4 distinct causes — and the test that matches each one
This is the section every other perimenopause-fatigue article skips. Each cause below has a specific biological mechanism, a specific lab test that screens for it, and a specific treatment. The reason "just get more sleep / manage your stress / take a multivitamin" is bad advice is that it ignores all four mechanisms in favor of generic platitudes. Two or three of these usually run together. The right intervention follows from the test result, not from the symptom alone.
Why eight hours of sleep does not equal eight hours of rest
The single most common mechanism. Estrogen, progesterone, and cortisol normally orchestrate a predictable nightly cycle: estrogen modulates serotonin precursors involved in sleep onset, progesterone increases slow-wave (deep) sleep via GABA-A receptor activity, and cortisol stays suppressed through the first half of the night before climbing toward the cortisol awakening response. In perimenopause, all three of these become erratic. Estrogen swings widely within a single cycle. Progesterone declines unpredictably across the luteal phase. Cortisol's nightly suppression weakens. The net effect: REM sleep shortens, slow-wave sleep fragments, and middle-of-the-night awakenings increase — even when total time in bed is normal. Kravitz et al.'s 2003 SWAN data documented that 32-40% of perimenopausal women report sleep complaints, and Joffe et al. (2010) showed that polysomnography in this group reveals architectural disruption even when sleep duration looks fine on paper.
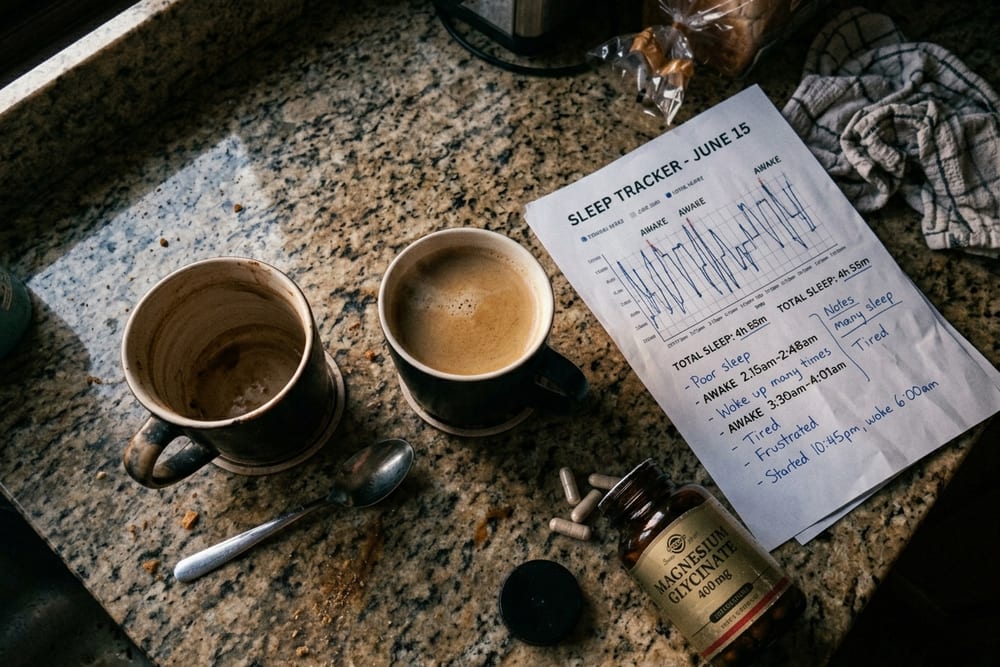
The clinical signature: you go to bed at 10:30, fall asleep within 20 minutes, "sleep" 8 hours, wake at 6:30 — and feel like you got 4. The duration is right; the architecture is wrong. Wearable sleep trackers often catch this pattern as a high "in-bed" number with low "deep" and "REM" totals, which is one diagnostic clue most clinicians never see because they don't ask. Hot flashes that wake you briefly without forming a conscious memory shred slow-wave sleep specifically, which is why women with night sweats are doubly affected.
Why your morning energy disappeared
The hypothalamic-pituitary-adrenal axis is the system that produces cortisol on a daily rhythm: highest at 7-9 a.m., dropping through the day, lowest around midnight. That morning peak is the biological alarm clock — it is what makes you feel awake, focused, and energized in the first hour after waking. In perimenopause, the cortisol curve flattens. The morning peak is lower; the evening trough is higher; the day-to-day variability increases. The downstream effect is that the hormonal alarm clock stops ringing, mornings stop feeling like mornings, and the natural energy gradient that used to carry you from breakfast to lunch evaporates.
Schmidt and Rubinow's (1991) review in Endocrine Reviews documented the bidirectional relationship between estrogen and HPA-axis function: estrogen modulates corticotropin-releasing hormone signaling and cortisol receptor sensitivity, and the loss of stable estrogen unfastens the system. The clinical signature: profound morning fatigue that paradoxically feels worse in the first hour after waking, sometimes a small mid-afternoon energy bump, and either a "second wind" at 9-10 p.m. or, more commonly, complete collapse by 8:30. Many women describe it as "wired and tired" — the system is hyperactive overall but lacks the rhythmic structure that produces useful energy.
The fatigue cause your CBC will miss
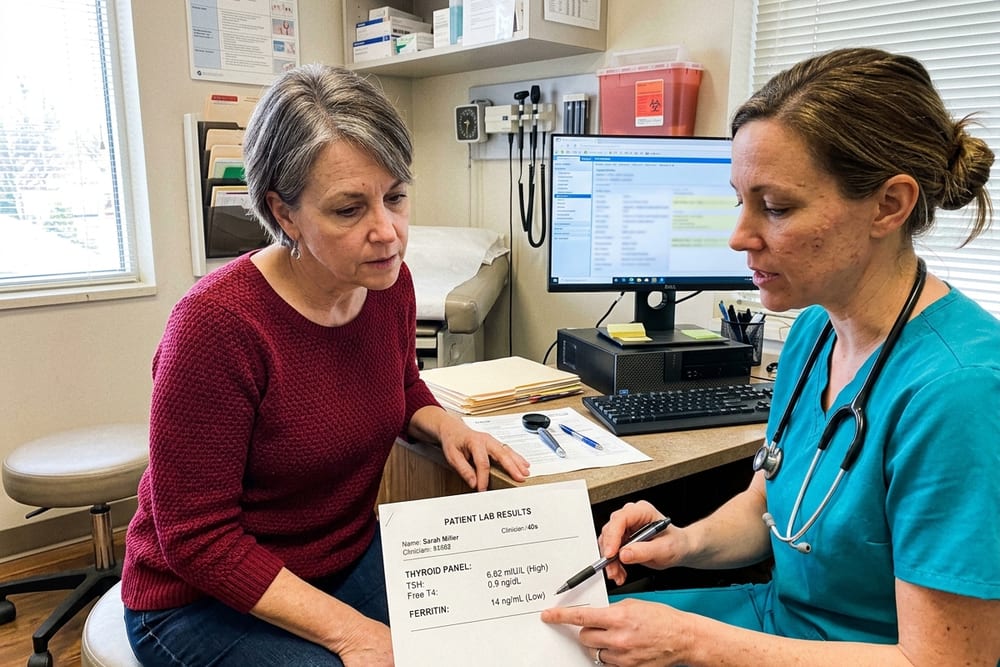
This is the most under-diagnosed cause on the list. Late perimenopause is characterized by erratic, often heavier menstrual bleeding — anovulatory cycles produce thicker endometrial linings, which shed in heavier flows. Punnonen and Rauramo's foundational 1980 work documented that perimenopausal women with heavy menstrual bleeding develop iron deficiency long before they develop frank anemia on a CBC. The reason is anatomical: ferritin (the body's iron storage protein) depletes first; transferrin saturation drops second; and only after months of sustained loss does hemoglobin fall below the conventional anemia threshold. So the standard primary-care workup — order a CBC, check the hemoglobin number, declare you "not anemic" — misses iron deficiency in its symptomatic-but-pre-anemic stage entirely.
The clinical signature: profound exhaustion, exercise intolerance, occasional restless legs at night, sometimes hair shedding, sometimes pica (a craving for ice or non-food substances), often pale conjunctiva on close inspection. The lab signature: ferritin in the 30-70 ng/mL zone — below the lab's "low" flag of around 15-30 but well below the energy-functional target of 70+ that menopause specialists use. This is the zone where you feel terrible and your lab report says "normal." A meaningful fraction of perimenopausal women presenting with fatigue have ferritin in this gray zone and have never been told.
The 3-to-5x increase in thyroid dysfunction nobody mentions
Schindler's 2003 paper in Maturitas and the subsequent body of work on perimenopause-thyroid intersection establish that subclinical hypothyroidism — TSH elevated above approximately 4.0 mIU/L with free T4 still within normal range — increases roughly 3 to 5 times in perimenopause compared with premenopausal age-matched controls. The presenting symptom is most often fatigue, not the textbook weight-gain-cold-intolerance pattern, because the thyroid dysfunction is mild and the system has had years to adapt. Hashimoto's autoimmune thyroiditis specifically clusters in midlife women, and the perimenopausal estrogen volatility appears to act as a trigger for previously-quiescent autoimmune thyroid disease in genetically susceptible women.
The clinical signature overlaps significantly with perimenopause itself — fatigue, sluggishness, mild cognitive fog, occasionally constipation, occasionally hair thinning at the lateral eyebrows. That overlap is exactly why it gets missed. A perimenopausal woman with fatigue is told her symptoms are perimenopausal; the thyroid never gets checked; or it gets a TSH-only screen that misses central hypothyroidism and the early antibody-positive Hashimoto's pattern.
The 4-test workup — what to ask your doctor for
Walk into your appointment with the four tests on a piece of paper. The reason this list matters is that "fatigue panel" is not a standard order — different clinicians order different things, and the perimenopausal-specific picture only emerges when all four are run together. If your clinician resists, ask which mechanism they think they are ruling out without each test. The conversation usually shifts.
| Test | What it screens for | Target / threshold | Why "in range" can still be wrong |
|---|---|---|---|
| TSH + free T4 | Subclinical hypothyroidism, Hashimoto's | TSH 1.0-2.5 functional; >4.0 abnormal | TSH alone misses central hypothyroidism; many labs flag only >5.0 |
| Ferritin | Iron storage depletion (pre-anemia) | >70 ng/mL for energy | Lab "normal" range often starts at 15-30; symptomatic deficiency commonly at 30-70 |
| Estradiol + FSH | Perimenopausal hormonal stage | FSH >25 mIU/mL suggests late perimenopause | Single time-point estradiol fluctuates wildly; trend matters more than one number |
| AM cortisol | HPA-axis function | 10-20 mcg/dL drawn 7-9 a.m. | Low-normal with morning fatigue is meaningful; absolute value alone misses curve flattening |
| Optional: thyroid antibodies (TPO, Tg) | Autoimmune thyroid disease (Hashimoto's) | Positive at any titer warrants follow-up | Often abnormal years before TSH crosses the threshold |
| Optional: salivary cortisol curve (4-point) | HPA-axis curve flattening across the day | Should peak 7-9am and decline through the day | More sensitive than single AM cortisol; rarely covered by insurance |
If two or more of these come back abnormal, that is not a coincidence — it is the perimenopausal-fatigue compounding pattern, and the treatment plan should address each axis individually rather than picking one. CBC alone, which is the default fatigue workup most clinicians order, screens for none of these except as a downstream proxy. Skip "I'm just tired, can you order some labs" and bring this list.
What actually helps perimenopause fatigue
The interventions below are mechanism-matched. Match the supplement, drug, or lifestyle change to the cause your workup uncovered, not to the marketing claim on the bottle. The first three address the largest causes; the next three are supportive; the last category is the money-pit you can stop spending on.
1. HRT — the systemic lever for the sleep and HPA arms
HRT is the single highest-leverage intervention for hormonal fatigue in this population because it addresses the two most common mechanisms — sleep architecture disruption and HPA-axis dysregulation — by stabilizing the estrogen volatility that drives both. Transdermal estradiol (patch, gel) or oral estradiol with progesterone if you have a uterus restores stable estrogen levels across the day; oral micronized progesterone at bedtime adds a deep-sleep-promoting GABA-A effect that is well-documented in the sleep-medicine literature. Most women report meaningful fatigue improvement within 4-8 weeks, in parallel with hot flash and sleep improvement. HRT does not directly fix iron deficiency or thyroid dysfunction — those need their own targeted treatment — but the slowing of heavy menstrual bleeding on HRT can indirectly improve ferritin status over months. Our companion piece on signs you need HRT walks through when this conversation is worth having.
2. Iron repletion — if ferritin is below 70 ng/mL
Ferrous bisglycinate 25-65 mg elemental iron daily is better-tolerated than the cheaper ferrous sulfate; both work. Take with vitamin C (orange juice or 250 mg ascorbic acid) for absorption; avoid coffee, tea, calcium, and antacids within 2 hours of the dose. Recheck ferritin at 3 months to confirm the trend. Most women see meaningful energy improvement within 8-12 weeks of starting iron, with full restoration of stores at 4-6 months. If oral iron is not tolerated or if ferritin is failing to climb, IV iron infusion is appropriate and increasingly available. Treating the cause of the heavy bleeding — often via HRT or progesterone — is part of the same intervention.
3. Thyroid treatment — if TSH is elevated and symptoms fit
Levothyroxine starting low (typically 25-50 mcg) and titrated by clinical response and repeat TSH at 6-week intervals. The functional target in symptomatic women is often TSH 1.0-2.5, lower than the lab's 0.4-4.0 "normal" range — because the lab range includes a substantial population of subclinical hypothyroid patients. Combination T4/T3 (levothyroxine plus liothyronine, or natural desiccated thyroid) is appropriate for the meaningful subset of women who do not feel well on T4 alone. Improvement timelines: cognitive fog often clears first at 4-6 weeks; fatigue at 6-12 weeks; full optimization at 6 months.
4. Strength training — counterintuitive but evidence-based
The instinctive response to bone-deep fatigue is to rest. Counter to the instinct, two or three weekly strength training sessions (45-60 minutes, compound movements like squat, deadlift, row, press) reliably reduces perimenopausal fatigue across multiple randomized trials. The mechanism is multifactorial: improved insulin sensitivity, mitochondrial biogenesis, modest cortisol-curve normalization, and improved sleep depth on training days. The catch is that you have to actually do it through the early-weeks slog when you feel worse before you feel better. Three weeks in is when most women turn the corner.
5. Magnesium glycinate at bedtime
Magnesium glycinate 200-400 mg about 30-60 minutes before bed has modest but consistent effects on sleep depth and night-waking frequency in perimenopausal women. The glycinate form is better-absorbed and less GI-irritating than magnesium oxide or citrate. It is supportive, not curative — magnesium does not fix the four mechanisms — but it is cheap, low-risk, and stacks reasonably with progesterone if you are on HRT.
DON'T waste money on these
- B-vitamin "energy drinks" and "energy" supplements. Most are caffeine plus high-dose niacin (which produces a flush often misread as "energy"). The B-vitamin doses are generic and rarely fix actual deficiency.
- Most "adrenal fatigue" supplement stacks. The underlying HPA-axis dysregulation pattern is real; the "adrenal fatigue" diagnosis as marketed by the supplement industry is contested in mainstream endocrinology. The products are largely placeholder ingredients (low-dose adaptogens, generic B-vitamins, licorice root) at sub-therapeutic doses.
- Generic multivitamins. They contain none of the targeted nutrients (iron, thyroid hormone, HRT-grade estradiol) at the doses that would actually move the needle on perimenopause fatigue.
- "Energy IV drips" at boutique clinics. Most are hydration plus B-12 plus saline at $200 a session. Hydration is fine; the rest is theater.
For the broader OTC-supplement audit, our top perimenopause supplements 2026 post evaluates the entire category by evidence level.

When fatigue is something else
Perimenopause fatigue is a specific cluster, but several other conditions present with profound exhaustion in midlife women and need to be on the differential. Get the 4-test workup, but also walk through these:
- Sleep apnea. Risk increases substantially in perimenopause as fat redistributes centrally and upper-airway tone changes with declining estrogen. Many women with perimenopausal weight redistribution are newly snoring and don't know it. Ask a partner or run an at-home sleep apnea test if you have any of: morning headaches, dry mouth on waking, witnessed apnea, or persistent fatigue despite a clean 4-test workup.
- Depression. Anhedonia, persistent low mood, hopelessness, and concentration problems alongside fatigue point toward depression. Many women have both depression and perimenopausal fatigue; treating the hormonal arm often unmasks how much of the picture was each.
- Chronic fatigue syndrome (ME/CFS). Diagnostic hallmark is post-exertional malaise — a 24-72 hour energy crash following physical or cognitive exertion. Distinct from perimenopausal fatigue, which often improves with movement.
- Hidden chronic infection. Long COVID, chronic Lyme, EBV reactivation. Worth considering if fatigue started suddenly after a viral illness or has neurological features (cognitive fog far out of proportion, autonomic symptoms).
- Sleep-disrupting medication or substance. Late-day caffeine, evening alcohol (suppresses REM), beta-blockers, certain antidepressants, late-day exercise. These can compound any of the four mechanisms.
Red flags that mean stop the perimenopause framing and call your doctor: sudden severe fatigue with chest pain, shortness of breath at rest, syncope, unintentional weight loss > 10 pounds, fever, lymphadenopathy, or fatigue with new neurological symptoms. None of these are perimenopausal. All warrant prompt clinical evaluation.
How ClearedRx prescribes HRT for perimenopause fatigue
ClearedRx is a doctor-supervised HRT service for women, online. You take a one-minute quiz. A licensed physician in our network reviews your symptoms and history within 24 hours. If you are a fit, they prescribe — and your treatment ships to your door, discreetly, the same week. We prescribe both compounded and FDA-approved HRT preparations; the patient picks based on cost, format preference, and clinical fit.
For perimenopause fatigue specifically, the formulation that matters is systemic HRT — transdermal estradiol patch or gel, oral or transdermal estradiol with progesterone if you have a uterus, or a compounded estrogen-and-progesterone body cream applied to thigh or arm. Oral micronized progesterone at bedtime is specifically useful for the sleep-architecture arm because of its GABA-A receptor effect. Local vaginal estrogen does not address the systemic mechanisms behind perimenopause fatigue and should not be substituted for systemic HRT for this purpose.
Most women who add systemic HRT for perimenopause fatigue see meaningful improvement within 4-8 weeks, in parallel with hot flash and sleep improvement. Cost framing the way our patients experience it: ClearedRx HRT starts at $49 per month for compounded preparations and $89 per month for FDA-approved generics, all-in (medication, doctor reviews, free shipping in all 50 states). New patients receive 50% off their first month. There are no surprise fees and no insurance paperwork. For broader cost context, our HRT cost comparison walks through every formulation across every channel. HRT addresses the sleep and HPA arms — the iron and thyroid arms still need their own targeted workup and treatment, which any reputable HRT clinician will encourage.

"Sleep difficulty during the menopausal transition is common, multifactorial, and frequently persists despite adequate sleep duration — implicating disrupted sleep architecture, vasomotor symptom intrusion, and altered HPA-axis function rather than insufficient sleep quantity alone." — Kravitz HM, et al. Sleep difficulty in women at midlife: a community survey of sleep and the menopausal transition. Menopause. 2003;10(1):19-28.
If you also want to map the rest of the picture
Perimenopause fatigue almost never travels alone. The same low-and-erratic-estrogen environment that drives sleep architecture disruption and HPA flattening typically also produces hot flashes, night sweats, mood changes, and the broader symptom cluster. Mapping the constellation is the cheapest diagnostic move you can make before deciding on a treatment lever. Our free Menopause Symptom Score is a 60-second self-check that scores the cluster as a single hormonal-fingerprint number. For the broader symptom catalogue, see our menopause symptoms overview; for the sleep arm specifically, our menopause insomnia page covers the architecture-disruption side, and our pillar 34 symptoms of perimenopause piece walks through the full picture. For sister-article context, our perimenopause vs menopause piece walks through which symptom-stage maps to which treatment, our signs you need HRT piece walks through when the conversation is worth having, our top perimenopause supplements 2026 piece audits the OTC category, our progesterone and sleep piece covers the bedtime-progesterone mechanism in depth, and our menopause statistics 2026 page has the prevalence numbers across symptoms.
Frequently asked questions
Why am I so tired in perimenopause?
Perimenopause fatigue is rarely one thing. It is four distinct biological mechanisms running in parallel: (1) sleep architecture disruption — estrogen and progesterone changes shorten REM and slow-wave sleep so even 8 hours of sleep is non-restorative; (2) HPA-axis dysregulation — the cortisol curve flattens and morning energy disappears; (3) iron and ferritin depletion from heavier perimenopausal periods, which depletes oxygen-carrying capacity before standard CBC anemia thresholds are crossed; and (4) a 3-5x increased rate of subclinical hypothyroidism in perimenopause. Each has a different treatment, which is why generic "sleep more, stress less" advice fails.
Can perimenopause cause severe fatigue?
Yes. The Study of Women's Health Across the Nation (SWAN; Kravitz 2003) documented that 32-40% of women in the menopausal transition experience moderate to severe fatigue interfering with daily function. Joffe et al. (2010) in Menopause showed perimenopausal fatigue often persists despite adequate sleep duration, because the underlying mechanism is not insufficient sleep but disrupted sleep architecture, flattened cortisol, depleted iron stores, or thyroid dysfunction. Severe perimenopause fatigue warrants the 4-test workup — TSH, free T4, ferritin, AM cortisol — before being attributed to lifestyle.
Does HRT help perimenopause fatigue?
Yes, for the sleep-architecture and HPA-axis arms specifically. Restoring stable estrogen smooths the volatility that disrupts REM and slow-wave sleep; oral micronized progesterone at bedtime has independent sedative and deep-sleep-enhancing effects via GABA-A receptor modulation. Most women report meaningful fatigue improvement within 4-8 weeks of starting HRT, in parallel with hot flash and sleep improvement. HRT does not directly fix iron deficiency or thyroid dysfunction — those need their own targeted treatment — but the slowing of heavy menstrual bleeding on HRT can indirectly improve ferritin status over time.
What blood tests should I get for perimenopause fatigue?
Four tests, not one: (1) TSH plus free T4 — TSH alone misses central hypothyroidism and the early-perimenopausal subclinical pattern; (2) ferritin — target above 70 ng/mL for energy, not just "in the lab range" (15-150); below 30 is overt deficiency; 30-70 is the sub-optimal-but-not-flagged zone where you feel terrible and the lab report says normal; (3) estradiol and FSH if menstrual irregularity suggests perimenopause stage; and (4) AM cortisol — drawn 7-9 a.m. before breakfast — to assess HPA-axis function. CBC alone is insufficient because hemoglobin can be normal while ferritin is depleted. Bring this list to the appointment.
Is bone-deep tiredness normal in perimenopause?
It is common but not "normal" in the sense of inevitable. The bone-deep, can't-be-fixed-by-coffee, can't-be-fixed-by-sleep tiredness women describe in perimenopause has a specific signature in the literature — Kravitz 2003 SWAN data and Joffe 2010 Menopause both document it, and both link it to disrupted sleep architecture rather than insufficient sleep duration. The pattern is often a mix of two or three of the four mechanisms (sleep architecture + HPA flattening, or sleep architecture + low ferritin) compounding each other. Most cases are treatable once the specific mechanism is identified — which requires the 4-test workup, not a generic "manage your stress" conversation.
Should I get my thyroid checked?
Yes. Schindler (2003) in Maturitas and subsequent reviews document that subclinical hypothyroidism — TSH elevated above 4.0 mIU/L with normal free T4 — increases roughly 3-5x in perimenopause, and that the presenting symptom is most often fatigue rather than the classic weight gain or cold intolerance. Standard practice is TSH alone, but for perimenopausal fatigue you want TSH plus free T4 plus thyroid antibodies if there is family history or any symptom cluster that fits Hashimoto's. Thyroid hormone replacement, when indicated, often resolves fatigue within 6-12 weeks.
What's the difference between perimenopause fatigue and depression?
They overlap but are mechanistically distinct. Depression is characterized by persistent low mood, anhedonia (loss of pleasure), guilt, hopelessness, and concentration problems alongside the fatigue; perimenopause fatigue more often presents with normal or only mildly affected mood but profound physical exhaustion that is worse in the morning, paradoxically often improves with movement, and clusters with hot flashes, sleep disruption, and irregular periods. The 4-test workup helps separate them — and so does the response to treatment. Perimenopause fatigue often improves on HRT plus targeted nutrient repletion; depression usually requires SSRIs, therapy, or both. Many women have both, and treating the hormonal piece often unmasks how much was depression versus how much was hormonal.
Can iron deficiency cause perimenopause fatigue?
Yes, and it is the most under-diagnosed cause on this list. Punnonen and Rauramo (1980) documented that perimenopausal women with heavy menstrual bleeding develop iron deficiency long before they develop frank anemia on CBC. The reason is that ferritin (the body's iron storage protein) depletes first, then transferrin saturation drops, and only after months of sustained loss does hemoglobin fall below the anemia threshold. Standard practice is to flag ferritin only if it is below 15-30 ng/mL, but symptomatic iron deficiency commonly presents at ferritin 30-70 — the zone where you feel exhausted and your lab report says "normal." Target ferritin above 70 ng/mL for energy. Iron repletion takes 3-6 months to fully restore stores.
How long does perimenopause fatigue last?
Untreated, perimenopause fatigue typically tracks the perimenopausal transition itself — 4-8 years on average — with worst severity in the late perimenopause window when estrogen swings are sharpest and ferritin depletion has had years to accumulate. With targeted treatment, the timeline collapses considerably. HRT improvements appear within 4-8 weeks; thyroid treatment within 6-12 weeks; iron repletion within 3-6 months; HPA-axis recovery within 8-16 weeks of sleep stabilization. Most women on a complete workup-and-treat protocol report meaningful improvement within 8-12 weeks and substantial resolution within 6 months.
What's the best supplement for menopause fatigue?
Honest answer: there is no single supplement that fixes perimenopause fatigue, because the cause is not a single deficiency. The interventions with the strongest evidence base are mechanism-matched: iron supplementation if ferritin is below 70 ng/mL; thyroid hormone if TSH is elevated; HRT for the sleep-architecture and HPA arms; magnesium glycinate at bedtime for sleep depth. The supplements to avoid: B-vitamin "energy drinks" that mostly contain caffeine plus high-dose niacin; most "adrenal fatigue" supplement stacks (the underlying diagnosis is contested in mainstream endocrinology and the products are largely placeholder ingredients); and generic multivitamins, which contain none of the targeted nutrients at therapeutic doses. Match the supplement to the test result, not to the marketing claim.
Sources & references
- Kravitz HM, Ganz PA, Bromberger J, et al. Sleep difficulty in women at midlife: a community survey of sleep and the menopausal transition. Menopause. 2003;10(1):19-28. PMID: 12544673
- Joffe H, Massler A, Sharkey KM. Evaluation and management of sleep disturbance during the menopause transition. Semin Reprod Med. 2010;28(5):404-421. PMID: 20613668
- Schmidt PJ, Rubinow DR. Menopause-related affective disorders: a justification for further study. Am J Psychiatry. 1991;148(7):844-852. PMID: 2026136
- Punnonen R, Rauramo L. The effect of long-term oral oestriol succinate therapy on the skin of castrated women. Ann Chir Gynaecol. 1980;69(3):133-136. PMID: 7436402
- Schindler AE. Thyroid function and postmenopause. Gynecol Endocrinol. 2003;17(1):79-85. PMID: 14559378
- The North American Menopause Society. The 2022 Hormone Therapy Position Statement of The North American Menopause Society. Menopause. 2022;29(7):767-794. PMID: 35797481
- Endocrine Society. Menopause and Hormone Therapy Clinical Practice Guideline (2024 update). endocrine.org
- Camaschella C. Iron deficiency. Blood. 2019;133(1):30-39. PMID: 30401704
- Andrews PW, Bharwani A, Lee KR, et al. Is serotonin an upper or a downer? The evolution of the serotonergic system and its role in depression and the antidepressant response. Neurosci Biobehav Rev. 2015;51:164-188. PMID: 25625874
- Internal: menopause symptoms overview · menopause insomnia · menopause statistics 2026 · menopause symptom score tool · 34 symptoms of perimenopause · perimenopause vs menopause · signs you need HRT · progesterone and sleep · top perimenopause supplements 2026
If you want to address the cause and not just the symptom — talk to a clinician
ClearedRx prescribes evidence-based HRT — bioidentical estradiol, progesterone, or a combined cream — based on your full picture, with 24-hour MD review and free shipping in all 50 states. Compounded preparations from $49/month, FDA-approved generics from $89/month. No insurance hassle. New patients save 50% on the first month.
Find out if HRT is right for me